Marijuana is the accepted term for Cannabis sativa, an herb with medicinal properties that is clinically proven to benefit cancer patients. Mesothelioma symptoms and treatment side effects often decrease a patient’s quality of life. For some patients, medical marijuana can provide relief from these conditions.
Learn more about alternative and complementary treatments that fight this disease.
Although the sale and use of marijuana as a recreational substance is a federal offense in the U.S., as of May 2024, it is approved in 24 states and the District of Columbia for recreational use and in 38 states for medicinal purposes — particularly for treating pain associated with cancer and for nausea and loss of appetite associated with chemotherapy treatment.
21%
Percentage of mesothelioma patients among survey respondents who use either medical marijuana or herbal medicine.
Source:
The Mesothelioma Center at Asbestos.com, 2023 Survey
Patients with mesothelioma cope with symptoms of the disease and side effects of cancer treatment such as chest pain and chemotherapy-induced nausea. A number of clinical trials found evidence that medical marijuana may help some patients manage cancer-related symptoms and side effects of cancer treatment.
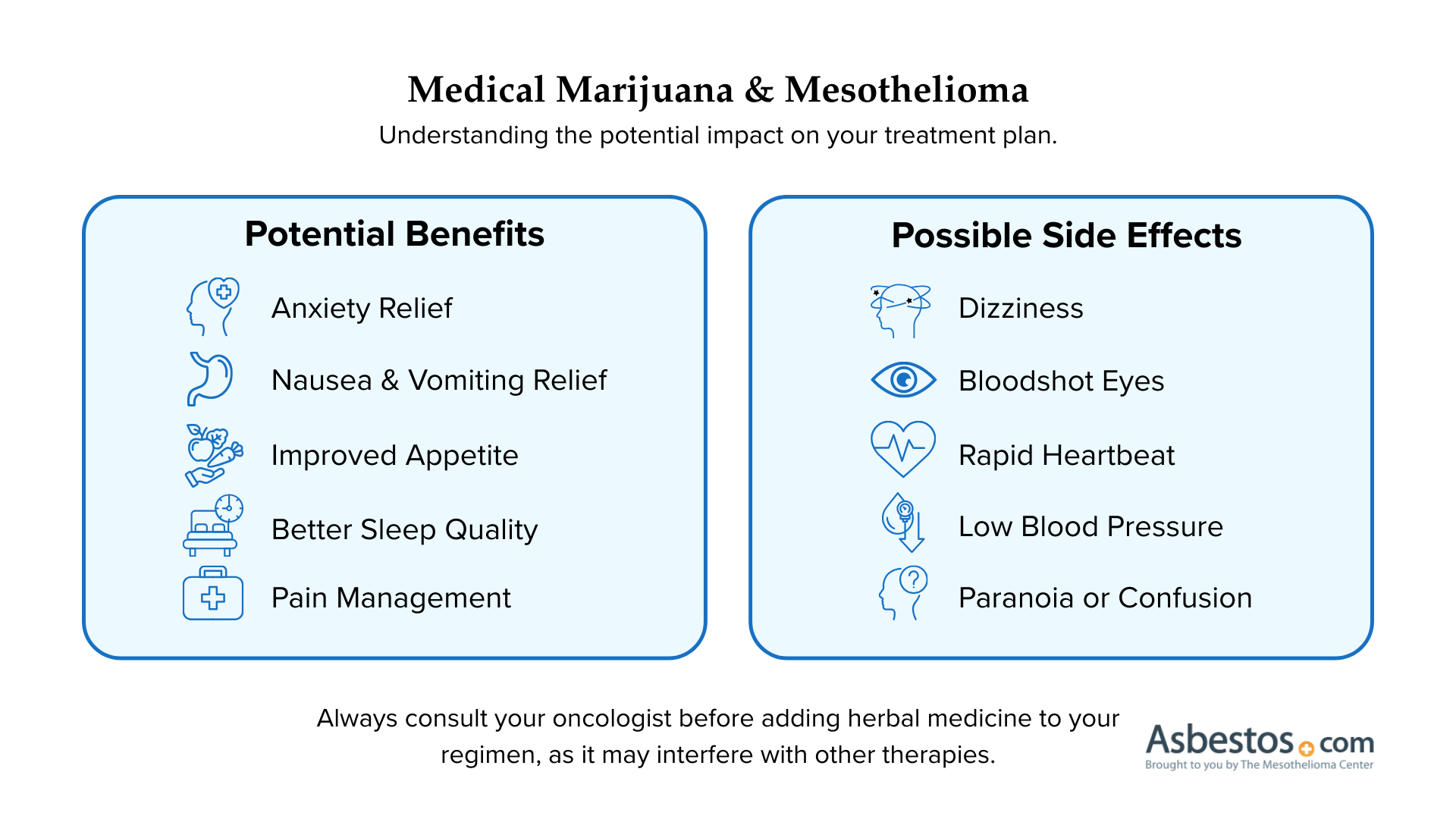
As with all forms of herbal medicine, patients should consult with their oncologist before using this type of complementary treatment because it may interfere with conventional treatments.
Benefits and Side Effects of Medical Marijuana
In clinical trials, medical marijuana was found effective for a range of symptoms associated with cancer treatment. Despite its benefits, medical marijuana may also cause side effects.
Benefits
Side Effects
Anxiety relief
Bloodshot eyes
Improved appetite
Dizziness
Improved sleep quality
Low blood pressure
Nausea relief
Paranoia
Pain relief
Rapid heartbeat
Reduced vomiting
Slowed food digestion
Patients report that side effects are generally mild, but vary depending on the strain of marijuana and how much is consumed. Researchers have not reported benefits or side effects of marijuana as a treatment for mesothelioma.
500+ SPECIALISTS AVAILABLE
Get to the Right Mesothelioma Cancer Center, Faster
Connect with top-rated mesothelioma specialists at a cancer center near you, who will personalize treatment options based on your diagnosis.
Scientific Research on Medical Marijuana in Cancer Care
Most of the scientific research on medical marijuana in cancer care has happened outside of the U.S. because marijuana remains illegal at the federal level. Growing support for the legalization of medical marijuana may promote cancer research in the future, but current research is limited in the U.S.
Global research efforts have increased in recent years because of a growing interest in the potential role of medical marijuana in cancer care. The research extends beyond the well-known tetrahydrocannabinol chemical, known as THC, to include other compounds, such as CBD, collectively known as cannabinoids.
Research on Cancer Symptoms and Treatment Side Effects
The bulk of medical research on medical marijuana and cancer has focused on how the herb may help patients cope with cancer symptoms and side effects of treatment. Different types of cancer-related pain, nausea, vomiting and sleep quality improved for a significant portion of participants in a number of studies.
Medical Marijuana Research in Cancer Care
2022: A Danish study surveyed 2,838 cancer patients who used cannabis during treatment and found 77% experienced at least one positive effect, while 33% reported at least one side effect. Less nausea and improved sleep were the most commonly reported effects.
2019: Expert Opinion on Investigational Drugs published a review of the medical literature on the use of medical marijuana in cancer care. It found evidence that it may help cancer patients cope with chemotherapy-induced nausea and vomiting, cancer-related pain, anorexia and cachexia syndrome, insomnia and anxiety.
2018: Current Pain Headache Reports published a review of randomized, controlled clinical trials involving medical cannabis for neuropathic pain, which is a common side effect of chemotherapy. Over the last 20 years, about a dozen clinical trials reported significant relief of neuropathic pain using marijuana over a placebo. The results and tolerability of marijuana for neuropathy was found comparable to prescription drugs.
2015: Cochrane Database of Systematic Reviews published a review of 23 randomized, controlled clinical trials involving cancer patients receiving medical marijuana for nausea and vomiting caused by chemotherapy. The study reported that patients receiving marijuana experienced less nausea and vomiting than patients receiving a placebo.
The Cochrane review also reported that marijuana controlled nausea and vomiting just as well as conventional anti-nausea drugs, and the patients who received both preferred marijuana over anti-nausea drugs. However, patients receiving marijuana were more likely to drop out of the trials because of side effects (such as dizziness or sedation) than patients receiving placebos or anti-nausea drugs.
Research on Medical Marijuana for Anti-Cancer Therapy
The research has looked at marijuana not only as a means to control cancer symptoms and treatment side effects but also as an anti-cancer therapy. Studies in test tubes and mice indicate that several types of cancer may respond to cannabis as an anti-cancer therapy. Some cancer cells die when exposed to cannabinoids, and some stop spreading.
Medical Marijuana and Anti-Cancer Therapy
2016: Research published in Progress In Neuro-Psychopharmacology & Biological Psychiatry found THC and other cannabinoids can kill cancer cells and limit their spreading. The study also noted research in animals that showed cannabis enhanced the effect of cancer drugs designed to stop tumor growth and spreading.
2016: A study published in Current Oncology found THC and CBD limited the growth of neuroblastoma in test tube studies and mice studies. Of the two cannabinoids, CBD was more active against this cancer.
2014: Oncotarget reported certain cannabinoid compounds in medical marijuana can kill a variety of cancer cells and block them from spreading. Researchers cited studies showing cannabinoids having anti-cancer effects in the following cancers: Lung, breast, prostate, skin, pancreatic, brain, bone, oral, thyroid and lymphoma.
It appears that certain cancer cells have cannabinoid receptors, but the precise function remains largely unknown. There isn’t enough research to know if marijuana affects mesothelioma tumor progression. Some mesothelioma survivors have used medical marijuana after conventional anti-cancer treatment and believe it contributed to their survival.
Cannabinoids May Promote Tumor Growth
It is important to note some laboratory research indicates cannabinoids may promote tumor growth in certain cancers. For example, a 2004 test tube study published in Cancer Research found THC promoted the growth of lung cancer and glioblastoma, a type of brain cancer.
A 2005 test tube study published in The Journal of Immunology found THC enhanced the growth and spreading of breast cancer. In 2000, the same journal published a study on mice with lung cancer and found THC accelerated tumor growth by limiting parts of the immune system that control cancer.
Further research in humans is required to fully understand how the chemicals in marijuana affect different types of cancer.
Edible Medical Marijuana
Patients with mesothelioma or lung cancer have weakened lungs and experience trouble breathing. For these patients, consuming edible marijuana may be preferable to smoking it to avoid aggravation of lung tissues.
There are some differences between smoked and edible marijuana. When marijuana is inhaled, the effects are felt almost immediately. When eaten, it takes longer to take effect because of the digestive process. The effect can take from 20 minutes to two or more hours to be fully felt, but the average time is around 90 minutes.
Many patients find the psychoactive effects of edible marijuana are milder and the body relief is stronger. This is sometimes more effective for cancer patients who seek relief from physical symptoms. The effects may also last longer.
Types of Edible Medical Marijuana
The most popular and most recognizable forms of edible marijuana are baked goods. Items such as brownies and cookies are made with cannabis-infused butter. Hash oil or hash-infused butter tends to have a higher concentration of marijuana, so less cannabis can be used, making the flavor milder. This type of marijuana can also be made into chocolates.
Other edibles include hard candies, cold drinks and teas. It is important to follow dosing instructions carefully and not overeat marijuana edibles. Patients are recommended to start with a very small dose to gauge the effects.
For patients who are watching calories, fat or sugar, there are alternatives to heavy baked goods. Tinctures are placed under the tongue for a short amount of time and then swallowed. According to some patients, the effect of tinctures is less sedating than edibles made with cannabis butter, and it is absorbed more quickly. Cannabis capsules usually contain a mix of cannabis and other oils, or other oils infused with cannabis. Patients take these like they would any other pill.
For patients who don’t prefer edibles, topical marijuana products are becoming more widely available. Topical products are primarily used to reduce body pain and inflammation in the area they are applied. This may help mesothelioma patients experiencing cancer-related pain such as chest pain or bone pain caused by growing tumors. Some states that haven’t enacted medical marijuana laws allow the sale of non-psychoactive cannabinoid products such as CBD topical creams.
FREE EXERCISE GUIDE
Boost Your Energy During Treatment
Doctor-approved exercises to help mesothelioma patients maintain strength and manage treatment side effects.
Since marijuana is not readily available to many patients, drug companies have developed synthetic versions of THC, the psychoactive ingredient in marijuana.
Types of Synthetic THC
A synthetic form of THC called dronabinol was approved by the U.S. Food and Drug Administration (FDA) as an appetite stimulant and for nausea. Brands include Marinol and Syndros.
Cesamet (nabilone) is another drug that contains a synthetic cannabinoid similar to THC that was approved to treat nausea and vomiting caused by chemotherapy.
Patients who have tried synthetic and natural versions of marijuana often say marijuana in its natural form is more effective for symptom relief than the synthetic variety. Marinol and Cesamet can also have serious side effects that aren’t a risk with natural THC, including seizures, irregular heartbeat, vision changes, headaches and severe or persistent dizziness.
Regulation and Legalization of Medical Marijuana
Regulations on marijuana began in the early 1900s. In 1970, the Controlled Substances Act classified marijuana as a Schedule I substance having “no accepted medical use.”
The country’s attitude toward medical marijuana began to shift in the late 1970s. In 1978, the National Institute on Drug Abuse (NIDA) supplied seven patients with marijuana after their physicians applied for the Expanded Access (compassionate use) program.
Legislation That Regulated and Criminalized Marijuana
Harrison Narcotics Act
Marihuana Tax Act of 1937
Boggs Act
Narcotics Control Act
Controlled Substances Act
In 1991, 53% of oncologists agreed that marijuana should be available by prescription and 66% said it helped cancer patients treat the side effects of chemotherapy.
The New England Journal of Medicine published an editorial calling for the rescheduling of marijuana in 1997. In 2008, the American College of Physicians stated that it supported non-smoked THC. The organization also called for an exemption from criminal prosecution for patients.
Exclusive Content
Kevin Hession: The Alternative Mesothelioma Treatments I Have Taken
This is our journey.
If you have mesothelioma, this is your journey.
You decide what your treatment is going to look like.
There’s a treatment I haven’t discussed at this point in time yet that I think is worthy of discussing at least to some degree. Now, it’s a little bit controversial.
I will open up this by saying if you like this as an idea, that’s an approach you need to consult with your healthcare provider. But I take acupuncture.
I I I go to a acupuncture called Doctor. China in Jacksonville, Florida.
And he he does a couple of things to me, but he was up upfront with me from the very beginning. He basically said, I cannot cure you if you’re mesothelioma.
What I can do is help you with some of the effects of some of the treatment that you’re receiving.
So, he does something called fire cupping which I would say doesn’t hurt but is uncomfortable when you’re going through it. And I’ve been going through it every Friday for the last four years. And what fire cupping does is it it puts pressure on your back and it allows for toxins in your body to be released and be eliminated from the body.
Why is this important? If you’re taking chemo, you have a certain amount of toxicity going through your body right now.
I am.
This helps alleviate some of the toxicity in my body.
Now, there’s risk associated with this and the risk that I understand it to be is that it does accelerate things going in your lymphatic system.
That’s where talking to a health professional, would come into play.
But I’m living evidence.
I’ve had thirteen CAT scans, no evidence of the disease. I’ve been able to tolerate all of my, chemo sessions.
Now I do have one, one net effect that I I haven’t really talked about yet either. And one of the things that help helps me with my chemo is a steroid.
On a scale of one to ten, the worst case of nauseousness I’ve ever had, on a scale of one to ten with ten being horrible and one being just enough to register had about I had one case where it was a three.
I owe that to the, the steroid that I’ve been receiving. Now over time, I guess that builds up something that’s also something you’re introducing to your body that your body probably doesn’t like. So I I now have what’s called steroid flush.
And usually a day or two after I have had my infusion, my face will turn bright red. Yes, it has and they’ve reduced the dosage that I’ve been receiving so it’s not quite as traumatic as it was when it first started surfacing.
But the bottom line is it allows me to tolerate the chemo that I’ve been receiving. And by receiving the chemo, that’s allowed me to live.
So that’s an important thing. So when you’re looking at your treatment, sometimes talking to your healthcare professional about other types of treatment whether it be what’s normal kind of treatment like, steroid, or something that might be different than treatment that you might receive otherwise like acupuncture.
Sometimes they might be answers that might be part of your journey.
States That Have Legalized Recreational Marijuana
Recreational marijuana became legal to purchase in Colorado and Washington in 2014. Since then, a total of 24 states, 3 territories and the District of Columbia have approved recreational marijuana.
States With Recreational Marijuana Laws
Alaska
Arizona
California
Colorado
Connecticut
Delaware
District of Columbia
Illinois
Maine
Maryland
Massachusetts
Michigan
Minnesota
Missouri
Montana
Nevada
New Jersey
New Mexico
New York
Ohio
Oregon
Rhode Island
Vermont
Virginia
Washinton
Washington
The legalization of recreational marijuana in these states involved removing prohibitions against the use, possession and sale of cannabis for non-medical purposes. Proponents say it reduces crime, generates tax revenue, allows better regulation and makes it more accessible to patients without a necessary prescription. Opponents raise concerns about the potential health impacts and increased usage, particularly among young people.
States That Have Legalized Medical Marijuana
After California legalized the drug in 1996, other states followed. Presently, 38 states, the District of Columbia, Guam, Puerto Rico and the U.S. Virgin Islands have legalized medical marijuana.
State
Possession Limit
Alabama
70 daily dosages at one time
Alaska
1 oz usable; 6 plants (3 mature, 3 immature)
Arizona
2.5 oz usable; 12 plants
Arkansas
2.5 oz usable per 14-day period
California
8 oz usable; 6 mature or 12 immature plants
Colorado
2 oz usable; 6 plants (3 mature, 3 immature)
Connecticut
2.5 oz usable
District of Columbia
2 oz useable; 6 plants (3 mature, 3 immature)
Delaware
6 oz usable
Florida
35-day supply (amount not specified)
Hawaii
4 oz usable; 10 plants
Illinois
2.5 oz of usable cannabis during a 14-day period
Kentucky
30-day supply
Louisiana
30-day supply
Maine
2.5 oz usable; 6 plants
Maryland
30-day supply; no more than 120 grams (approximately 4 oz)
Massachusetts
60-day supply (10 oz)
Michigan
2.5 oz usable; 12 plants
Minnesota
30-day supply of non-smokable marijuana
Mississippi
3 oz per month
Missouri
6 oz per month
Montana
1 oz usable; 4 plants (mature); 12 seedlings
Nevada
2.5 oz usable; 12 plants
New Hampshire
2 oz of usable cannabis during a 10-day period
New Jersey
2 oz usable
New Mexico
6 oz usable; 16 plants (4 mature, 12 immature)
New York
30-day supply of non-smokable marijuana
North Dakota
3 oz per 14-day period
Ohio
Maximum of a 90-day supply; amount to be determined
Oklahoma
8 oz in a residence; 3 oz in public
Oregon (only state to accept out-of-state applications)
24 oz usable; 24 plants (6 mature, 18 immature)
Pennsylvania
30-day supply
Rhode Island
2.5 oz usable; 12 plants
South Dakota
3 oz
Utah
113 grams of unprocessed cannabis
Vermont
2 oz usable; 9 plants (2 mature, 7 immature)
Virginia
4 oz per 30-day period
Washington
8 oz usable; 6 plants
West Virginia
30-day supply
Medical marijuana laws establish systems for cultivating, distributing and prescribing cannabis to people with specific conditions. Each state has different laws on which medical conditions qualify, but in general, people with cancer are eligible in each of these states.
Consult Your Oncologist About Medical Marijuna
If you live in a state that offers medical marijuana, ask your oncologist how it might benefit or interfere with your treatment plan. People assume it couldn’t hurt to take a natural substance, but cannabis products contain antioxidants that may protect cancer cells from the wanted effects of chemotherapy and radiation therapy.
This means certain types of medical marijuana might have the potential to block your anti-cancer treatments from working properly. Your oncologist is your best resource for guidance on this matter.
A number of mesothelioma survivors have said they spoke with their doctor before using medical marijuana as a complementary therapy to conventional treatment, which is known as integrative oncology.
Medical Marijuana Experiences for Mesothelioma Survivors
One mesothelioma survivor, Andy Ashcraft, said he used cannabis oil for years and believed it helped him cope with mesothelioma. His wife and caregiver thoroughly researched how to dose and administer cannabis oil to cancer patients before Andy began taking it.
Another survivor, Pete K., said he used edible medical marijuana to lessen the side effects of chemotherapy.
California resident and mesothelioma survivor Jim Huff said he uses cannabis oils to control his cancer and promote sleep.
While research shows medical marijuana may help cancer patients cope with pain, nausea, anxiety, lack of appetite and insomnia, it is best to discuss how you want to use marijuana with your doctor to get their approval first and make sure you take the right product, at the right time, without interfering with your treatment plan.
Recommended Reading
Your web browser is no longer supported by Microsoft. Update your browser for more security, speed and compatibility.
If you are looking for mesothelioma support, please contact our Patient Advocates at (855) 404-4592
Fact Checked
Our fact-checking process begins with a thorough review of all sources to ensure they are high quality. Then we cross-check the facts with original medical or scientific reports published by those sources, or we validate the facts with reputable news organizations, medical and scientific experts and other health experts. Each page includes all sources for full transparency.
Reviewed
Asbestos.com is the nation’s most trusted mesothelioma resource
The Mesothelioma Center at Asbestos.com has provided patients and their loved ones the most updated and reliable information on mesothelioma and asbestos exposure since 2006.
Our team of Patient Advocates includes a medical doctor, a registered nurse, health services administrators, veterans, VA-accredited Claims Agents, an oncology patient navigator and hospice care expert. Their combined expertise means we help any mesothelioma patient or loved one through every step of their cancer journey.
More than 30 contributors, including mesothelioma doctors, survivors, health care professionals and other experts, have peer-reviewed our website and written unique research-driven articles to ensure you get the highest-quality medical and health information.
About The Mesothelioma Center at Asbestos.com
Assisting mesothelioma patients and their loved ones since 2006.
Helps more than 50% of mesothelioma patients diagnosed annually in the U.S.
A+ rating from the Better Business Bureau.
5-star reviewed mesothelioma and support organization.
My family has only the highest compliment for the assistance and support that we received from The Mesothelioma Center. This is a staff of compassionate and knowledgeable individuals who respect what your family is experiencing and who go the extra mile to make an unfortunate diagnosis less stressful. Information and assistance were provided by The Mesothelioma Center at no cost to our family.
Whitmer, M. (2026, March 9). Medical Marijuana and Mesothelioma. Asbestos.com. Retrieved July 27, 2026, from https://www.asbestos.com/treatment/alternative/medical-marijuana/
MLA
Whitmer, Michelle. "Medical Marijuana and Mesothelioma." Asbestos.com, 9 Mar 2026, https://www.asbestos.com/treatment/alternative/medical-marijuana/.
Chicago
Whitmer, Michelle. "Medical Marijuana and Mesothelioma." Asbestos.com. Last modified March 9, 2026. https://www.asbestos.com/treatment/alternative/medical-marijuana/.
Most helpful, steered us in the right direction for treatment. Great source of information and support, the Center followed through on every one of our requests.
Because of their guidance, I was able to navigate getting my mother into MD Anderson when her case got put aside by mistake in all the COVID-19 craziness. Vanessa was amazing and I can’t recommend enough reaching out to them. I thought it was a gimmick to get you to hire a lawyer, but I was so wrong. They truly seemed to want to help meso patients and KNOW what you need to ask and do in order to get help.
Hearing the news about my mother's diagnosis was heartbreaking. I felt lost, I didn't know how I could help or where to seek the best medical care. I started researching specialists online and shortly after, Dr. Smart reached out to me. She has been extremely helpful and encouraging throughout this entire process. Even though we aren't located in her area, she has helped us get in contact and set up appointments with the best doctors/specialists nearby. She has always been available for any questions that we have, and she even sent us a binder full of helpful resources. The patient advocates are amazing and true to their title. Dealing with this process is not easy, but knowing that we have someone like Dr. Smart in our corner is reassuring and we are so grateful for her and The Mesothelioma Center.
My son Carlos was diagnosed with this terrible and unknown disease a few months ago. Thank God we found The Mesothelioma Center along the way, and Vanessa Blanco who provided us with information on hospitals and doctors who have been of great help. I am very grateful to them.
Extremely communicative and helped my dad get an appointment with one of the top centers in Philadelphia. I'm so grateful for this center. They assisted with information on nutrition, legal help, and scheduling appointments. Special thanks to Danielle!
Danielle DiPietro was an invaluable resource for me. Her suggestions and recommendations guided us towards stellar practitioners in our area. Without her advocacy, I feel we would have been receiving less-than-optimal medical and legal care for mesothelioma. Receiving the diagnosis was a shock and I felt lost initially. I wish everyone could take advantage of this FREE assistance.
I was very grateful and appreciative of Dr. Smart from The Mesothelioma Center. She was very helpful to my husband and me. She educated and walked us through the steps, and suggested ideas and questions to ask his doctors. She also provided me with a lot of information that I can read and educate myself about this illness. We need more people like Dr. Smart, who is very educated and you can tell she enjoys the work that she does by the way she assisted my husband and me. We thank the Lord and are grateful that we met Dr. Smart from The Mesothelioma Center.
In January of 2016, my husband was diagnosed with peritoneal mesothelioma. Our first reaction was: what is this and what can we do? He was diagnosed by an oncologist and was scheduled to start chemotherapy. When we arrived home that day, I googled mesothelioma and discovered The Mesothelioma Center had a form to fill out to request additional information. I filled it out and within an hour, I received a phone call from Karen Selby from The Mesothelioma Center asking if I needed any help. Karen was and still is my lifeline. She located a doctor at the Cleveland Clinic who performed surgery and HIPEC on peritoneal mesothelioma patients. My husband was scheduled with an appointment and his surgery was performed on March 3, 2016. He continued with follow-up appointments with the oncologist until a friend of ours passed away from it in 2017. Immediately I sent Karen an email asking if she knew any mesothelioma specialists at the clinic, and of course, I got a prompt response back with a name. Everything was going well until the last CAT scan, which showed it returned. He is now doing chemo and has his next CAT scan scheduled for the end of March with a follow-up for the results with the mesothelioma doctor. Without Karen, I am not sure my husband would still be here. She provided me with so much information along with help in various ways, too numerous to even mention. Thank you to all those who are there to help us.
Registered and Licensed Dietitian & Contributing Writer
Tejal Parekh is a registered and licensed dietitian in Florida. As a writer for The Mesothelioma Center at Asbestos.com, the nation's most trusted mesothelioma resource, she uses her knowledge of nutrition to help mesothelioma cancer patients.
Fact-checked and verified content:
Our fact-checking process begins with a thorough review of all sources to ensure they are high quality. Then we cross-check the facts with original medical or scientific reports published by those sources, or we validate the facts with reputable news organizations, medical and scientific experts and other health experts. Each page includes all sources for full transparency.
Please read our editorial guidelines to learn more about our content creation and review process.